The Gap Limiting The Gain
Why Your Longevity Plan Will Break At The Point of Care

Systems Longevity Series · Essay I of IV

Executive Summary
The longevity industry is currently experiencing a state of “industrial decoherence,” where advancements in biological planning and financial modeling have outpaced the physical and systemic infrastructure required to support an aging population. While individual planning for lifespan, healthspan, and wealthspan has reached unprecedented levels of sophistication, the “Carespan”—the capacity of the environment to provide timely, skilled care during life transitions. Remains the weakest link in the longevity chain.
Critical Takeaways:
The Coherence Gap: There is a widening disparity between “sick care” (clinical/emergency response) and “care” (transition infrastructure such as rehabilitation and home support).
Systemic Failure Points: By 2040, the OECD forecasts a shortage of 13.5 million long-term care workers. Current systems are failing not due to a lack of clinical evidence, but a lack of operational capacity.
The Carespan Framework: Longevity is comprised of five spans—Lifespan, Healthspan, Wealthspan, Workspan, and Carespan. Carespan is the “coupling variable” that determines whether the other four spans survive a health crisis or transition.
The Dual Casualty Effect: Care infrastructure failure creates two victims: the individual requiring care and the informal caregiver (often a family member), whose own health, career, and financial trajectories are derailed by the lack of formal support.
Economic Impact: Unpaid caregiving in the U.S. is valued at $600 billion annually, far exceeding total out-of-pocket healthcare expenditures.
This essay is the first in a four-part series on Systems Longevity, which proposes that longevity is not just a characteristic of individuals, but also of the systems they are part of. The first essay identifies the main problem: the gap between how well we plan for longevity and how well care is actually delivered. It starts by looking at care infrastructure, which is the most obvious and immediate point of failure in the longevity system. However, the series goes beyond this. The next essays take a broader view, moving from healthcare to the complete overhaul of societal systems, including housing markets, economies, financial structures, and social contracts, which is necessary when people live a generation longer than expected. What starts as a question about care delivery becomes a question about everything we have built based on the old assumptions about human lifespan.
There’s never been a better time to plan for a long life. Biological age testing has become much more accurate. Precision nutrition is now tailored to individual needs. Metabolic monitoring has improved significantly. Advanced financial modeling is more sophisticated than before. AI-augmented health coaching offers smarter insights than it did a decade ago.
In a mid-sized city, a 74-year-old is being discharged from hospital after just three days, following a hip fracture, because the rehab beds are full. Her daughter, coordinating from two states away, is told that a home care slot won’t be available for eleven days. The rehab facility her surgeon recommended has a six-week wait. The hospital is focused on managing its patient flow, but no one is focused on managing her recovery.
The plan existed. The evidence for what she needed existed. The infrastructure to deliver it did not.
The longevity industry faces a stark reality: its care infrastructure, comprising workforce, facilities, home care, and coordination, is not evolving to meet the needs the population they serve. Care workers in wealthy countries are leaving their jobs at an alarming rate, outpacing new hires and exacerbating staffing shortages. By 2040, the OECD forecasts a staggering shortage of 13.5 million long-term care workers, a deficit that no country is currently equipped to fill. Meanwhile, urban centers are monopolizing specialist care, abandoning rural and suburban communities with inadequate support. The disparity between the lofty promises of longevity planning and the harsh realities of care delivery is escalating, demanding immediate attention and reform.
This is not just about funding. Many high-income countries already invest heavily in aged care. The main issue is a lack of capacity, driven by structural, demographic, and escalating challenges. The longevity industry, focused on optimization and extension, has largely overlooked this capacity problem.
The outcome is a gap between elaborate longevity plans and the actual care provided. When this gap becomes clear, such as during a crisis or when significant changes are needed, it creates major issues. It triggers a chain reaction, rather than a minor problem, and demands attention.
The Wrong Question
The longevity industry has organized itself around a question: How long can we live? Adjacent to it: How much do we need to fund a long life? These are reasonable starting points. But they are incomplete framings that have systematically misdirected both individual planning and institutional investment.
They are trajectory questions. They assume the main challenge of a long life is its duration and cost. They believe that if you extend the timeline and fund it properly, the system will hold together effectively. What they miss is the architecture question: Does the system have the capacity to sustain itself through the transitions that a long life inevitably produces?
Living a long life means navigating a path with many obstacles. Falls, diagnoses, surgeries, and personal losses are just a few of the challenges people face. Each one puts the surrounding environment to the test, showing whether it can help the person recover or make their situation worse.
What ultimately determines the outcome is not how carefully someone planned for the future or how much they saved for retirement. It’s the actual care they receive when they need it most. This care should be available, skilled, and provided in a timely manner, taking into account the person’s daily life and surroundings.
This is the insight most longevity frameworks have missed. And it requires a distinction that changes everything.
Care is not the same as sick care. Sick care happens after someone gets ill and it’s unavoidable - it’s the emergency response, the clinical procedure, and the treatment. Care, in a broader sense, is different altogether.
When you think about it, care infrastructure includes all the systems that need to work well as people live, work, save, and retire over a longer period. This affects many areas, such as housing markets that assume people will downsize at 65 and pass away at 82. It also affects labor markets that rely on younger generations taking over jobs from older ones. Tax systems are based on working people supporting retired people, but the ratio of workers to retirees is changing. Social contracts were written with a different understanding of what a long life means. All these areas are part of care infrastructure - they either help people thrive over a long life or fail to.
This essay zeroes in on the health delivery layer, the weakest link in the care system transition infrastructure, to shed light on a larger issue. The Systems Longevity series as a whole takes aim at a more profound problem: the urgent need to overhaul our health systems. These were based on old demographic assumptions that are no longer valid and are now failing.
Within this larger context, the key distinction in this essay is one that the longevity industry often overlooks. Care, even in the limited sense of health delivery, is not the same as sick care. Instead, it serves as transition infrastructure, determining whether the system can withstand a shock or break under it. This infrastructure decides whether a person can regain their footing or lose their way. It determines whether the years following a crisis are marked by restored function or a downward spiral.
The difference between these two outcomes rarely depends on the quality of the initial clinical treatment. More often, it hinges on the quality of what follows - rehabilitation, home support, care coordination, and the recovery environment. This is what care truly entails. Yet, it is precisely this aspect of care that is being rationed, delayed, or substituted as the capacity gap grows wider.
Abstract Capacity Meets Operational Reality
At AlphaSage, our research on industrial decoherence reveals a troubling trend: America’s intelligence capabilities are outpacing its physical infrastructure, causing a growing mismatch. As we plan with increasing sophistication, our operational infrastructure deteriorates, leading to a predictable failure pattern (the growing mismatch between planning sophistication and physical infrastructure capacity. See webpage for more information, here). The fault line emerges where advanced planning meets inadequate physical resources, consistently resulting in breakdowns at the point where abstract ideas meet real-world implementation.
The longevity system is following this same pattern of failure.
Return to that hip fracture. The clinical evidence has been clear for decades: Richard Asher documented the dangers of bed rest in 1947, and the research has only grown stronger since. A 2019 meta-analysis across multiple studies found that hospital-associated disability — measurable functional decline caused not by the original illness but by the hospitalization itself . Affects approximately 30% of older adults admitted for acute care, a figure that has remained stubbornly consistent despite shorter hospital stays (Growdon et al., JAMDA 2019; anchored by Gill et al., JAMA 2010). Early, high-quality post-acute rehabilitation dramatically changes that outcome. Hospital-at-home models lower mortality and readmission rates compared to traditional care. This conclusion comes from 42 randomized controlled trials with nearly 7,000 patients. The U.S. Centers for Medicare and Medicaid Services also confirmed this in their 2024 study of the Acute Hospital Care at Home initiative.
The knowledge exists. The protocols exist.
For the 74-year-old in that hospital bed, the issue is not a need for more evidence, but rather a need for a system that can effectively use the evidence we already have. In many places, the system is failing because it lacks the necessary resources, including sufficient staff, adequate facilities, and proper coordination. This is not a problem of uncertainty, but of capacity. Until we address this shortfall, we will continue to see patients experiencing decline, institutionalization, and other poor outcomes that could have been prevented with better care.
The Five Spans — and the One That Holds Them Together
Consider your life as a whole, divided into five key areas that work together. These areas depend on each other and form a system. When this system is strong, it helps you through difficult times. When it’s weak, it can fail you.
Lifespan is the container — total biological duration, the timeline within which everything else must remain functional.
Healthspan is the quality of those years — functional vitality, biological resilience, the physical and cognitive capacity to act on a long life rather than merely endure it.
Wealthspan is the financial layer — not just retirement savings, but the dynamic capacity to fund prevention, housing adaptation, and the transitions between life stages. Wealthspan is less a savings problem than an exposure management problem, and care costs are the most undermodeled exposure in most financial plans.
Workspan is meaningful contribution — purposeful engagement in work, creativity, mentorship, and community. It is both a longevity driver (purpose and cognitive engagement are among the strongest predictors of healthspan outcomes) and, as we will see, a longevity casualty when the system fails.
Carespan is the fifth domain, and it is architecturally different from the others.
The distinction is worth clarifying before proceeding. The first four variables are primarily individual in nature, influenced by personal choices, habits, and planning decisions. In contrast, Carespan is a coupling variable, representing the interaction between the individual and their environment. This concept forms the basis of the PeakOS longevity framework, and notably, it is a dimension that most longevity plans fail to consider.
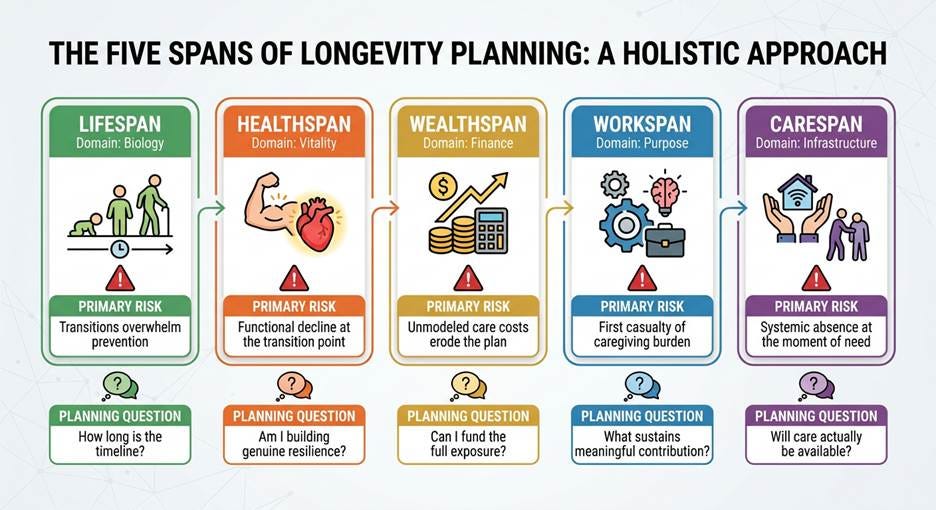
Systemic absence at the moment of need
Will care actually be available?
That final row is the one most longevity plans leave blank. Carespan has two dimensions that must be assessed separately.
Personal carespan is what you can influence: your care network and relationships, the suitability of your home for aging in place, your advance care planning documents, and the resilience of your informal caregiving relationships.
Systemic carespan is largely outside your control: the geographic availability of care services where you live, the capacity of the care workforce in your region, the waitlist exposure you face, and the institutional readiness of local systems to serve the population they will soon face.
This distinction matters enormously. You can have a strong personal carespan, with documented wishes, a committed care network, and a thoughtfully modified home, yet still face a systemic carespan failure if the formal infrastructure around you collapses under demographic pressure. The plan relies on a supportive environment, but that environment may not be in place.
That is what makes carespan the critical variable in the framework. It cannot be fully internalized by individual planning. It is the condition on which all the other spans depend when disruption arrives.
The Cascade
When carespan fails at a transition moment, the consequences do not stay bounded. They propagate across every other span simultaneously.
A fall, a diagnosis, or a cognitive shift can disrupt anyone’s longevity plan. The key to recovery is what happens next. If a person gets the right care at the right time, they can stay independent, keep functioning, and keep working towards their goals. This care must be available, competent, and timely, and it should happen in the setting the person prefers.
When this care is in place, the person can absorb the disruption and get back on track. Their healthspan continues, and their wealthspan is protected from big losses. They can go back to work or adapt to a new situation, and their longevity plan stays on course.
But when care is not available, things can go badly wrong. If rehabilitation is delayed, home support is missing, or discharge is rushed, the disruption gets worse. The person’s functioning declines, and they may lose their independence. They may even need to be institutionalized. This can lead to huge, unexpected costs that were not planned for. The person’s workspan may end, and years of investment in their health and financial security can be wasted. The cost of this gap in care is very real and should be included in every longevity plan. It can mean expensive institutional stays, avoidable readmissions, or years of decline that could have been prevented with proper care. These are not just minor issues - they are major financial events that matter.
The cascade does not begin at the moment of illness. It begins at the moment the care system fails to absorb it.
The Dual Casualty
There is a second consequence of Carespan failure that longevity planning almost entirely ignores: the caregiver becomes a longevity casualty alongside the person being cared for.
Meet someone who exists in some form in almost every family. She is 58. She has spent thirty years building a career in financial services, and the last decade building the retirement savings that were meant to fund her own long life. She runs five mornings a week. She has her own financial planner. She has, by most measures, done everything right.
Eighteen months ago, her mother had a stroke. The formal care system offered twelve hours of funded support per week. The waitlist for more was fourteen months. So she stepped in, first part-time, then more, then fully. She has reduced her hours at work. She has stopped exercising most weeks. She is exhausted in ways she does not have language for. Her own health, financial, and career trajectories are quietly unwinding.
One Carespan failure. Two longevity casualties.
The numbers tell a compelling story: 63 million Americans, or one in four adults, are now caregivers for older adults or people with serious illnesses, according to the National Alliance for Caregiving and AARP’s 2025 report. This represents a significant increase of 20 million caregivers since 2015. The demands of caregiving are substantial, with the average family caregiver devoting 25 hours per week to unpaid care. As a consequence, many working caregivers must make difficult choices, such as reducing their work hours or leaving the workforce temporarily, with 16 percent having done so, as reported by AARP and S&P Global in 2024. The economic implications are equally striking, with the annual value of unpaid caregiving estimated at $600 billion in the United States, far surpassing total out-of-pocket health care expenditures, as noted in AARP’s 2023 research.
These caregivers are not a peripheral population. They are the backbone of the long-term care system. And the longevity planning industry is, for the most part, modeling them out of existence.
The hidden cost of treating care infrastructure as an afterthought does not just affect the person who needs care. It also affects the people around them, quietly reducing their lifespan and impacting those who are most invested in their well-being.
What Coherent Longevity Planning Looks Like
The shift required here is a reorientation of the primary question.
Not: How long can I live, and how much will it cost?
But: How do I maintain coherence across a longer timeline? Does the environment I inhabit have the capacity to support that coherence when the transition moments arrive?
This reorientation means different things depending on where you stand.
For individuals, adding carespan to your longevity assessment means more than just a checklist. It’s about truly evaluating the operational reality. Where do you live, and what care is actually available there? Who is in your care network, and what is their realistic capacity over the next decade? Have you had the family conversation about caregiving preferences before a crisis forced it? Is your home genuinely suitable for aging in place, or does it silently compound your risk if function declines? These are not soft questions. They are the questions that determine whether your other planning survives contact with reality.
For financial advisors and planners, the care cost line in your model is the least important part of the carespan problem. The more significant risks are capacity risk (will care be available?), setting risk (will it be delivered where the client wants it?), and caregiver risk (does the plan implicitly depend on an informal carer whose own longevity trajectory is not in the model?). We must include these financial variables in our analysis of longevity risk and sequence-of-returns risk. Relying on a spouse or sibling for unpaid care puts both their financial security and yours at risk. However, current plans only account for one person’s risks.
For investors, The carespan gap is a structural market failure - it’s not a temporary dip that will fix itself. It’s a growing gap between the demographic reality and the ability to deliver care. The OECD predicts a nearly 30% rise in long-term care demand by 2050. This increase is driven by aging populations and the weakening of informal family support networks that usually provide care. That gap will not be closed by the market forces currently in play.
The opportunity is real and underpriced. Hospital-at-home models have shown better outcomes than institutional care in many randomized trials, but they still lack enough funding compared to their proven potential. AI-augmented care coordination could change the economics of a system limited by its workforce, but technology takes decades to scale, not years. Meanwhile, the demographic wave of the 2030s is approaching. A strategic investment in the workforce, emphasizing training, compensation, and retention for care professionals, is long overdue. Supplementing this effort with robotic and automated care solutions can revolutionize the system’s economics, yet the pace of implementation and associated costs must be carefully managed to ensure a successful rollout.
The 63 million Americans currently providing unpaid family care represent both a neglected market and a largely invisible economic risk. When that cohort reduces its workforce participation — and the data shows clearly that it does — the cost lands not just on individual families but on employers, pension systems, and national productivity. That is not a soft consideration. It is a balance sheet problem that has not yet found its balance sheet.
To maximize returns, the longevity economy requires a robust care infrastructure to support extended healthspan. Each dollar invested in healthspan extension without a corresponding investment in care delivery infrastructure is unlikely to yield its full potential when the critical transition moment arrives.
The Coherence Imperative
The longevity industry has done remarkable work on the intelligence layer. We have made great progress in understanding the biology of aging, healthspan, and the financial aspects of a long life. We now know more about these things than ever before.
However, the systems and environments that provide care when it’s needed have not improved at the same rate.
This difference is called the coherence gap. To close it, we need to think of care infrastructure as the foundation of the entire longevity system, rather than just a cost to be managed later.
Before checking your health markers, consider whether the care system in your area can support you after a serious health issue. Before planning your retirement income, think about who will care for you and what that will cost them. Before investing in the longevity economy, ask if the necessary infrastructure is in place to deliver on its promises.
The question was never only how long.
Not longer. How long can it be sustained.
This is the coherence imperative at the heart of Systems Longevity.
Next in the series: Essay II — Care Entropy and the Aging System
A Living Simulation
To explore this, I built an interactive system and website:
👉 [Peak OS Systems Longevity — Interactive Demo]
👉 [Systems Longevity — Interactive Website]
<iframe src=”https://claude.site/public/artifacts/83ce7f8f-57f9-4133-9f74-b4e405722b97/embed” title=”systems-longevity-v2.html” width=”100%” height=”600” frameborder=”0” allow=”clipboard-write” allowfullscreen></iframe>
Selected Sources
Esposito N. “Care Access: The Missing Link in Longevity Planning.” LinkedIn Pulse. 2025. https://www.linkedin.com/pulse/care-access-missing-link-longevity-planning-nadine-esposito-ospfe
Browne L. “Peak OS for Professionals: The Hierarchy of Intervention.” AlphaSage · Substack. 2025. https://substack.com/@lasallebrowne/p-186712165
Browne L. “Longevity Doesn’t Need More Data. It Needs an Operating System.” AlphaSage · Substack. 2025. https://substack.com/@lasallebrowne/p-186056141
Gill TM, Allore HG, Gahbauer EA, Murphy TE. Change in disability after hospitalization or restricted activity in older persons. JAMA. 2010;304(17):1919–1928.
Growdon ME, Shorr RI, Inouye SK. Prevalence of Hospital-Associated Disability in Older Adults: A Meta-analysis. Journal of the American Medical Directors Association. 2019.
OECD. Who Cares? Attracting and Retaining Care Workers for the Elderly. OECD Health Policy Studies. 2020.
OECD. Social Economy in Care with a Focus on Ageing. 2024.
National Alliance for Caregiving and AARP. Caregiving in the US 2025. July 2025.
AARP. Valuing the Invaluable: 2023 Update. AARP Public Policy Institute. 2023.
AARP and S&P Global. Working Caregivers Report. 2024.
Centers for Medicare and Medicaid Services. Fact Sheet: Report on the Study of the Acute Hospital Care at Home Initiative. September 2024.
Shepperd S et al. Hospital in the Home: a meta-analysis. Medical Journal of Australia. 2012. (42 RCTs, n=6,992)
LaSalle Browne is the founder of AlphaSage, working at the intersection of AI systems architecture, industrial strategy, and geopolitical theory. The PeakOS longevity framework is an AlphaSage initiative.
© 2026 AlphaSage. This essay may be shared with attribution.
The dual casualty effect is a huge strain on our society. A few years ago, my mom was sick and she passed away from early-onset Alzheimer's, and watching my father manage her care was its own kind of slow devastation. There was no satisfying infrastructure to lean on. We looked. Ultimately, we handled it out ourselves, the way most families do, but it wasn't easy at all. Really important piece, LaSalle. Thanks for tagging me.